You've built something valuable. Maybe it's a digital health service, a specialist clinic, a diagnostics platform, or a product that solves a real operational problem. The problem isn't always the offer. It's that nobody outside your immediate circle trusts it yet.
That's the hard truth in healthcare communications. Good intentions don't carry much weight. Neither does a glossy launch release full of adjectives. Patients want clarity. Journalists want evidence. Clinicians want accuracy. Regulators want you to stay within the lines. Investors and partners want proof that your story will hold up under scrutiny.
That pressure is amplified in Britain because healthcare communications sit in the long shadow of the NHS, created in 1948 and still the central reference point for public expectations about care, access and accountability. The NHS remains the UK's largest employer, with around 1.7 million staff in England alone, and it handles approximately 1.3 million patient contacts every 24 hours across GP appointments, hospital services and community care, according to the World Health Organization overview of primary health care. In that environment, even a local service change can become a national trust story.
That's why effective PR for healthcare has to work like journalism first and marketing second.
At Carlos Alba Media, that newsroom mindset is built in. Everyone working on accounts is either a former national news journalist or has agency experience with international brands. That matters because the quickest way to lose a healthcare story is to pitch it like an advert. The quickest way to earn attention is to understand how editors think, what producers cut, what legal teams fear, and what a hostile interview sounds like before it happens.
Your Starting Point for Healthcare PR Success
Most healthcare organisations start in the wrong place. They begin with what they want to say rather than what the outside world needs to hear.
A founder will often arrive with a product deck, a claims sheet and a list of features. None of that is useless. It's just incomplete. A journalist won't ask whether your platform is cutting-edge. They'll ask whether it solves a recognised problem, whether the claim is evidenced, who benefits, what the limits are, and why this matters now.
Start with the public interest test
The first question isn't, “What are we launching?” It's, “Why should anyone beyond our office care?”
That means pressure-testing your story against a small set of questions:
- Who is affected: Patients, clinicians, commissioners, employers, or a specific underserved group?
- What changes: Access, speed, clarity, safety, operational burden, or patient understanding?
- What evidence supports it: Published material, service data, policy context, expert commentary, or documented outcomes?
- What can't be claimed: Anything that overreaches clinical evidence or implies guaranteed outcomes.
If you can't answer those cleanly, the story isn't ready.
Practical rule: If your first paragraph sounds like investor language, rewrite it until a health correspondent can explain it to a reader in plain English.
Build for scrutiny, not applause
Healthcare PR is different from lifestyle PR because the downside risk is higher. A weak consumer campaign may underperform. A weak healthcare campaign can attract legal concern, regulator attention, reputational damage, or the kind of coverage that defines your organisation for the wrong reasons.
That's why starting well means doing three things before any outreach begins:
Define the claim
Keep it narrow. “We improve access to a specific service” is workable. “We are transforming healthcare” is not.
Name the audience
Don't lump everyone together. Patients, hospital managers, clinicians and policy stakeholders don't read the same outlets or trust the same evidence.
Choose the spokesperson
The most senior person isn't always the right media voice. The right spokesperson is the person who can explain complex topics clearly, stay calm under challenge, and avoid making new claims on air.
Think like the newsroom
Former journalists spot weak stories quickly because they've rejected them for years. They know what lands in an inbox and gets ignored. They know when a quote has been written by committee. They know when a press office is trying to hide uncertainty behind jargon.
A stronger starting point is to frame your communications around what a real editor would green-light:
| Weak approach | Stronger journalist-led approach |
|---|---|
| Product-first announcement | Problem-first story |
| Broad claims | Narrow, supportable claims |
| Corporate quote | Human, accountable spokesperson |
| Coverage volume goal | Trust and message accuracy goal |
That shift sounds simple. In practice, it changes everything from messaging to media targets to crisis handling.
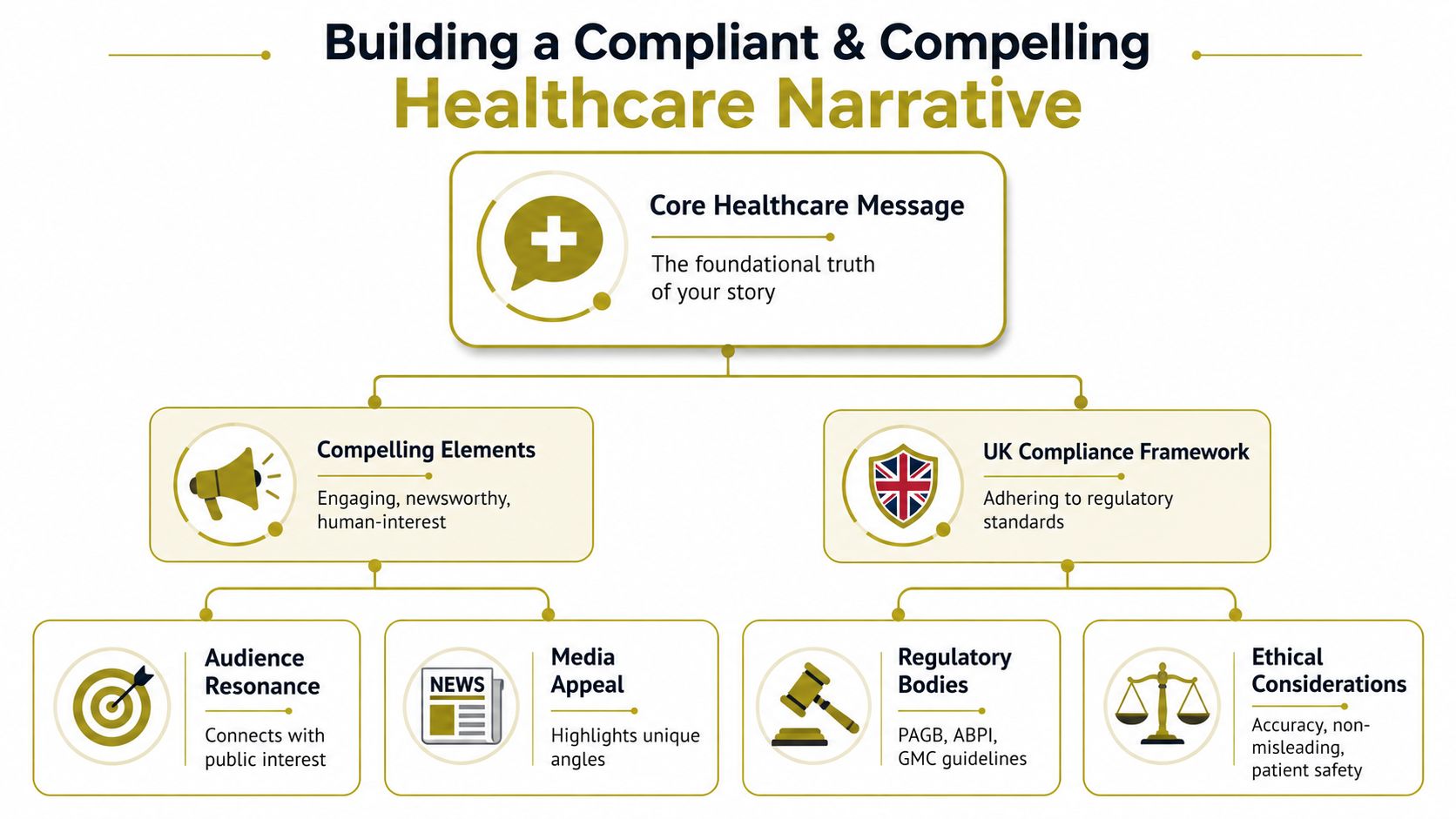
Building a Compliant and Compelling Message
A healthcare message has to do two jobs at once. It has to earn attention and survive checking. If it only does one, it fails.
The safest route is to build the narrative in layers. Start with the verified truth of what your organisation does. Then shape the human consequence of that truth. Only after that should you decide how to package it for press, social, web or stakeholder communications.
Use the three-part message test
A message is usually fit for healthcare PR when it clears these three tests.
Evidence
Every headline claim needs a source trail inside the business. That may include clinical material, service data, operating policies, approved wording, or expert review. If a spokesperson can say it publicly, someone internally should be able to substantiate it quickly.
Story
Facts alone don't travel. Journalists need tension, consequence and relevance. The useful question is not “What have we built?” but “What changes for a real person, service or system because this exists?”
Compliance
A story can be emotionally strong and still be unusable if it strays into misleading language. That happens when teams overstate benefits, flatten nuance, or imply that one service solves a broader system problem it doesn't control.
Move beyond generic patient benefit claims
One of the most underused routes in UK healthcare PR is access storytelling that doesn't stop at waiting list rhetoric. The public conversation is more complicated than “people need appointments faster”. It also involves geography, deprivation, referral pathways, local capacity and service awareness.
That matters because people living in the most deprived areas experience a much greater disease burden and worse access outcomes, as discussed in this analysis of underserved healthcare populations. If your messaging only says “we help patients”, you're probably missing the main concern.
A sharper narrative sounds more like this:
- Name the barrier: location, service awareness, referral friction, or limited specialist provision
- Explain your role: support, supplement, extend, or simplify
- State the limit: what you don't replace, what still requires in-person care, and where NHS pathways remain central
Better healthcare messaging often explains constraints as clearly as benefits.
That honesty usually improves coverage quality because it gives journalists something they can trust.
Make complex information easier to absorb
Healthcare buyers often need more than one format before they understand a proposition. A careful press release can open the door, but explainers often do the heavy lifting afterwards. Teams developing patient or stakeholder content can learn useful lessons from these animated healthcare video insights, especially when turning technical services into plain-English narratives.
The same principle applies to your wider planning. A message shouldn't sit in isolation from audience, channel and risk. If you're tightening the foundations first, it helps to map the story inside a broader communications strategy for regulated organisations.
What journalists actually look for
Editors and producers usually respond to a healthcare story when four things are obvious:
- The angle is current: It connects to a live public concern, policy issue, service challenge or trust debate.
- The claim is supportable: Nobody has to guess what sits behind it.
- The speaker is credible: Clinically informed where needed, plain-spoken, and accountable.
- The copy is clean: No inflated wording, no unnecessary jargon, no obvious legal loose ends.
A compelling healthcare message doesn't sound excited. It sounds clear.
Navigating the Media and Regulatory Gauntlet
Once the message is built, the actual work starts. This is the point where many organisations get stuck between legal caution, marketing ambition and newsroom deadlines.
A practical healthcare PR process needs discipline. Not because bureaucracy is admirable, but because healthcare stories can fall apart quickly when claims, approvals and media handling aren't aligned.
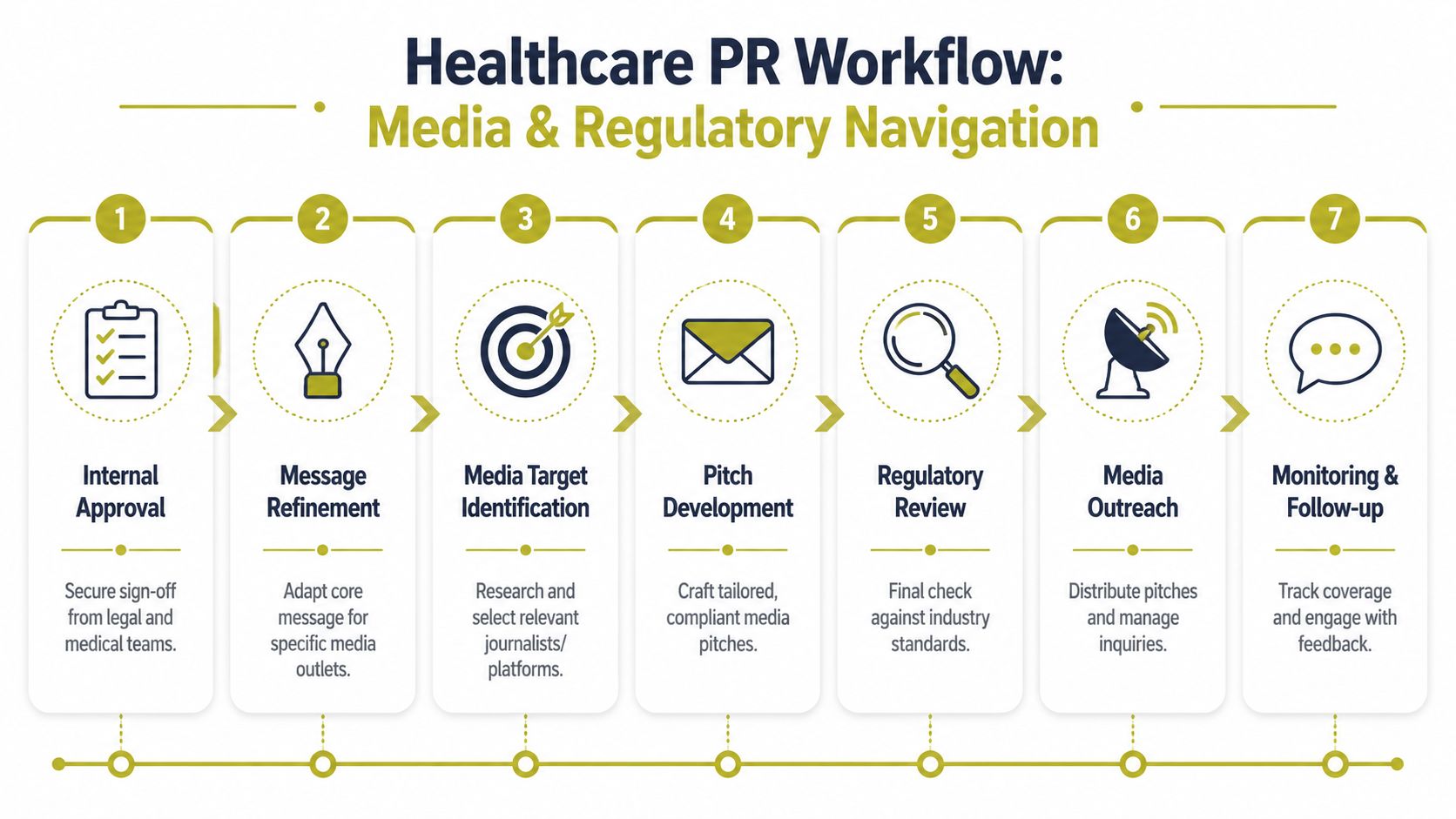
Build an approvals chain that can move
The worst system is one where nobody knows who signs off what. That's how deadlines are missed, journalists lose patience, and spokespeople end up improvising around unresolved wording.
A workable chain usually includes:
- Operational owner who confirms the service reality
- Medical or clinical reviewer where the subject touches patient care
- Legal or compliance check for claim wording and risk
- PR lead who adapts approved facts into media-safe language
- Spokesperson clearance so the person fronting the story knows the boundaries
Not every campaign needs the same level of review, but every healthcare campaign needs a named route to approval.
Pitch for authority, not volume
A lot of weak agencies still celebrate clip counts as if every mention carries equal weight. In healthcare, that's a mistake. A short, accurate piece in a trusted title can do more for credibility than a large pile of low-quality mentions.
That aligns with a practical benchmark from healthcare analytics thinking. Health data systems often struggle with interoperability and governance, which is one reason PR teams shouldn't rely on raw coverage numbers without quality control, as discussed in this piece on healthcare data and reporting pitfalls. The communications equivalent is simple. Count less. Judge better.
A newsroom-led targeting process usually prioritises:
| Priority | What to assess |
|---|---|
| Editorial trust | Is this outlet respected by the audience that matters? |
| Audience fit | Does it reach patients, clinicians, procurement teams, or policymakers? |
| Claim tolerance | Will the publication demand a high standard of evidence? |
| Format suitability | Is this best as comment, case-led feature, interview, op-ed, or broadcast hit? |
Handle cynical editors like a reporter would
Editors are sceptical because they should be. They've seen overblown launches, selective data, shaky spokespeople and PR teams who vanish when the difficult questions begin.
So pitch accordingly.
- Lead with the true angle: Don't bury the public-interest line beneath company boilerplate.
- Offer proof early: Put the supportable claim up front and make background material easy to access.
- Acknowledge limits: If there are constraints, say so. Qualified honesty often increases trust.
- Prepare for the hostile question: “How is this different from a private shortcut?” “Does this widen inequality?” “Are you replacing clinicians with technology?” Those questions aren't unfair. They're predictable.
The strongest healthcare pitch often includes the answer to the editor's first objection before they ask it.
Keep a live evidence file
Experienced teams save time. For every campaign, maintain a single working file that includes approved language, substantiation, spokesperson notes, likely challenge points, and rapid-response lines for incoming queries.
That file is especially useful when a story moves from print to broadcast or when social media picks up one line and strips it of context. The underlying facts need to stay stable even as the format changes.
Amplifying Your Story with Digital PR and SEO
Healthcare communications no longer end when a piece lands in the press. In many cases, that's when the harder reputation work begins. People search. They compare. They screenshot. They ask whether the story stands up once it leaves the headline and enters Google, LinkedIn, AI summaries and message boards.
That's why digital PR and SEO matter so much in healthcare. They aren't separate from trust. They are part of trust.

Treat discoverability as reputation management
Healthcare is a high-scrutiny category. If your organisation appears in search with thin pages, vague author attribution, weak explanations and unsupported claims, users notice. So do journalists doing background checks.
A stronger digital footprint usually includes:
- Expert-led articles that answer real questions in plain English
- Clear authorship so readers know who is speaking and why they're qualified
- Evidence-aware wording that avoids straying into medical promises
- Consistent message architecture across website copy, media coverage and social posts
Healthcare brands often make a mistake by publishing SEO content as if volume alone will solve visibility. It won't. In regulated sectors, low-trust content can create more problems than silence.
Build content that can survive AI summaries
Healthcare PR now operates in an information environment shaped by AI, misinformation and rapid interpretation. The UK government's 2024 to 2025 health policy agenda includes expanding digital tools in the NHS, and that has sharpened discussion around trust, safety and evidence standards, as noted in this policy commentary on healthcare access and public policy. For communicators, the implication is clear. PR is shifting from simple media coverage to risk-managed explanation.
That means your online content must answer difficult questions directly:
- What does the technology do?
- What does it not do?
- How is data handled?
- Where is human oversight?
- Does digital access replace face-to-face care, or support it?
If those answers aren't on your site, other people will answer for you.
A lot of teams are also trying to understand the impact of AI search on marketing, because brand visibility increasingly depends on how information is interpreted and surfaced, not just indexed.
Use digital channels to reinforce authority
LinkedIn, owned media and search-led content work best in healthcare when they echo the same disciplined message used in press work. The format can change. The standard shouldn't.
A useful operating model looks like this:
One core position
State the central claim once, in approved language.
Multiple proof formats
Support that claim with articles, explainers, executive commentary, FAQs and short social assets.
One source of truth
Keep wording aligned across site copy, social captions, PR materials and spokesperson notes. If a journalist checks your site after an interview, they shouldn't find a bolder claim there.
This short video is a useful prompt for thinking about visibility, format and search behaviour in a more joined-up way.
For organisations that need day-to-day alignment between press work and owned channels, social planning matters as much as search planning. A joined-up PR and social media approach helps prevent the common problem where media messaging sounds careful but the brand's social output sounds loose.
Mastering Crisis Preparedness and Media Training
Most healthcare organisations don't think clearly about crisis communications until something has already gone wrong. By then, time has gone. Screenshots exist. Internal disagreements spill into public view. A founder is asked for comment before a proper line has been agreed.
That's avoidable.
Crisis planning in healthcare should assume that pressure will arrive fast and often from more than one direction at once. A complaint can become a journalist enquiry. A digital product concern can become a data question. A staffing issue can become a safety story. A misleading social post can become evidence of a wider governance problem.
Prepare before the first call comes in
A sensible crisis plan doesn't need to be long. It needs to be usable.
The essentials are straightforward:
- List your pressure points: complaints, service disruption, data concerns, clinician conduct, advertising wording, AI claims, patient access concerns
- Name the response team: who approves, who speaks, who monitors, who liaises with lawyers
- Write holding lines in advance: short, factual statements that buy time without sounding evasive
- Set an escalation threshold: know what triggers legal review, board awareness or round-the-clock media handling
If you don't have that in place, build it before the next product update, funding announcement or service launch. This practical guide to developing a crisis communications plan covers the operational side in more detail.
“No comment” is rarely a strategy. In healthcare, it often reads as disorganisation.
Media training is not optional for founders
Founders sometimes assume media training is about polishing performance. It isn't. It's about reducing risk while keeping authority intact.
A healthcare spokesperson needs to be able to:
| Pressure moment | What trained spokespeople do |
|---|---|
| Challenging interview | Answer directly, then bridge back to approved ground |
| Incomplete information | Acknowledge what's known and what's being checked |
| Loaded accusation | Stay calm, avoid defensiveness, separate fact from allegation |
| Technical misunderstanding | Translate without patronising or overexplaining |
Untrained spokespeople often make one of two mistakes. They become too guarded and sound evasive, or they relax and overstate. Both are dangerous.
Rehearse the hard questions, not the easy ones
The best prep sessions don't focus on the introduction. They focus on the ambush.
Ask your spokesperson the questions a sceptical journalist would ask:
- Why should patients trust this?
- What evidence sits behind that claim?
- Does this benefit everyone equally?
- Are you shifting burden back onto patients?
- Is technology replacing clinical judgement?
That rehearsal matters because confidence in healthcare interviews doesn't come from charisma. It comes from knowing where the facts end, where the risks sit and how to stay useful under pressure.
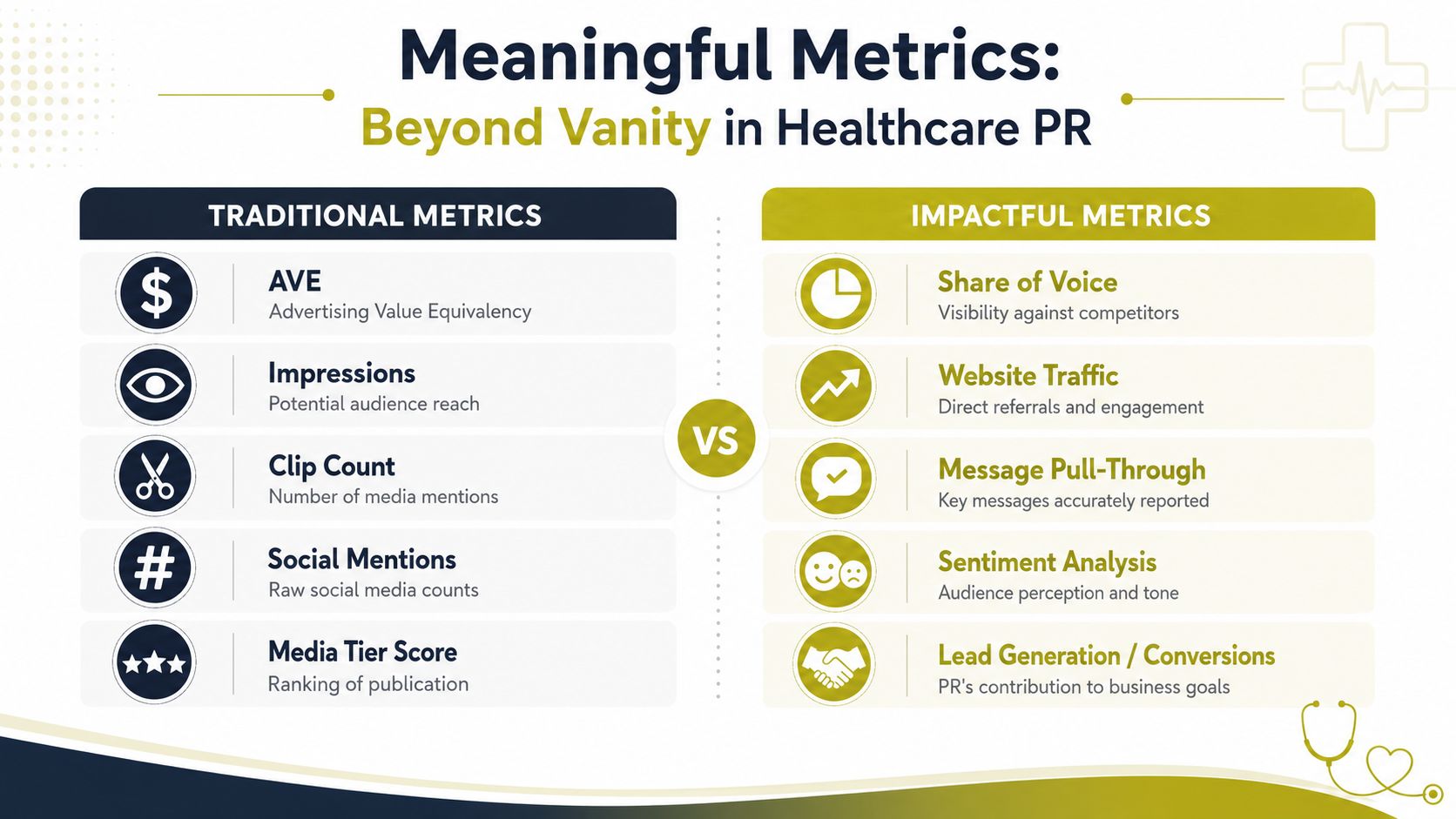
Measuring What Matters in Healthcare PR
A lot of healthcare PR reporting still hides behind numbers that look tidy but don't help anyone make decisions. Clip counts, reach estimates and inflated value comparisons may fill a slide deck, but they don't tell a chief executive whether the work changed anything meaningful.
The better approach is stricter. Decide what outcome matters before the campaign starts. Then measure against that outcome using a source trail you trust.
That's consistent with quality-improvement guidance, which stresses that teams must agree the problem definition and use a universally agreed metric because metric validity matters as much as the data itself, according to the National Library of Medicine guidance on quality improvement and measurement.
Start with one primary KPI
Not ten. One.
If the campaign exists to generate qualified enquiries, use that as the primary KPI. If the purpose is clinician sign-ups, use that. If it's message recall among a specialist audience, define how you'll test that before launch.
Then build supporting metrics around the journey, not around vanity.
A practical framework looks like this:
- Primary outcome: the one business or communications result that matters most
- Message accuracy: whether the core point appeared correctly in coverage
- Referral quality: whether people arriving from coverage took useful action
- Audience fit: whether the right stakeholders saw the story, not just a large audience
- Conversion evidence: whether awareness translated into a next step
Separate awareness from commercial impact
Many reports struggle with this distinction. A campaign may create visibility without producing commercial movement. It may also generate the right kind of trust before conversion appears later. Those are not the same thing, and they shouldn't be bundled together.
A cleaner dashboard separates them.
| Awareness measures | Outcome measures |
|---|---|
| Quality coverage | Qualified enquiries |
| Message pull-through | Booking clicks |
| Trusted outlet placement | Clinician interest |
| Audience relevance | Contact form completion |
That structure helps leadership understand whether the issue is media quality, landing-page performance, offer clarity, or internal follow-up.
Validate before you celebrate
Healthcare data is messy. Inputs can be incomplete, inconsistent or manually captured in ways that distort the picture. That's why PR teams should be cautious about broad claims built on weak attribution or unclean reporting.
Good measurement discipline usually means:
- Set a baseline before outreach
- Standardise tags and naming conventions
- Check source integrity before reporting
- Review anomalies rather than smoothing them away
- Keep campaign claims separate from assumptions
If you can't explain where the number came from, don't put it in the report.
For regulated organisations, this matters twice. First because leadership needs reliable evidence. Second because any public-facing success claim can itself become a reputational risk if the underlying data won't stand up to challenge.
The point of measuring healthcare PR isn't to prove that activity happened. It's to prove that the right activity moved the right audience towards the right action.
If your organisation needs a journalist-led approach to PR for healthcare, Carlos Alba Media provides senior counsel across media relations, digital strategy, crisis communications and media training, with work handled by former national news journalists and experienced agency professionals who understand both the newsroom and the regulatory pressure around healthcare stories.